By Aeruxo — Licensed flight dispatcher (study guide) | 15+ Years in Airline Operations
The ACARS message came in at 14:37 KST.
EMER DESCENT INITIATED. CABIN ALT UNCONTROLLED. SQUAWKING 7700.
I had been tracking that aircraft — a narrowbody on the Seoul–Osaka sector — for the last hour. Now the altitude readout was dropping fast. 35,000 feet. 32,000. 28,000. The crew wasn’t calling yet. They were busy: masks on, thrust levers back, nose down, descent checklist running. ATC was already clearing the airspace below them.
I had 60 seconds to do my part of the job before they’d need anything from me.
In 15 years working airline operations control, I’ve tracked three rapid decompression events in real time. This is what I know about what actually happens — on the flight deck, in the cabin, and in the OCC — during those first critical minutes.

What you need to know up front:
- Rapid decompression is survivable. In every case I’ve tracked, passengers landed safely at a divert airport. The system is designed to work.
- You have 18 seconds of useful consciousness at cruise altitude without oxygen. That’s why the mask comes before everything else — including the person next to you.
- The emergency descent, not the masks, is what actually resolves the emergency. The masks exist to keep you conscious long enough for the descent to work.
- The crew knows exactly what to do. They’ve practiced this scenario more times than most pilots can count. Your job is simple: mask on, seatbelt fastened, follow instructions.
What “Rapid Decompression” Actually Means
Every commercial aircraft above 10,000 feet operates with a pressurized cabin. The air inside is artificially maintained at an equivalent of roughly 6,000 to 8,000 feet — comfortable for breathing even when the aircraft is at 37,000 feet. Rapid decompression is what happens when that pressurization fails faster than the system can compensate, and the interior starts equalizing toward the outside altitude.
The word “rapid” covers a wide range. At one end, there’s a gradual pressure loss — a door seal failure, a pressurization controller fault — that raises cabin altitude slowly over several minutes, giving the crew time to respond before passengers feel anything significant. At the other end is explosive decompression: a structural failure — a window, fuselage panel, or cargo door — that equalizes pressure in a fraction of a second with a loud bang, a rush of air, and a sudden drop in temperature.
Cinema has fixed the explosive version in public imagination. In actual operations, pressurization system malfunction is the more common cause. Both trigger the same crew response.
The 18 Seconds That Explain Everything
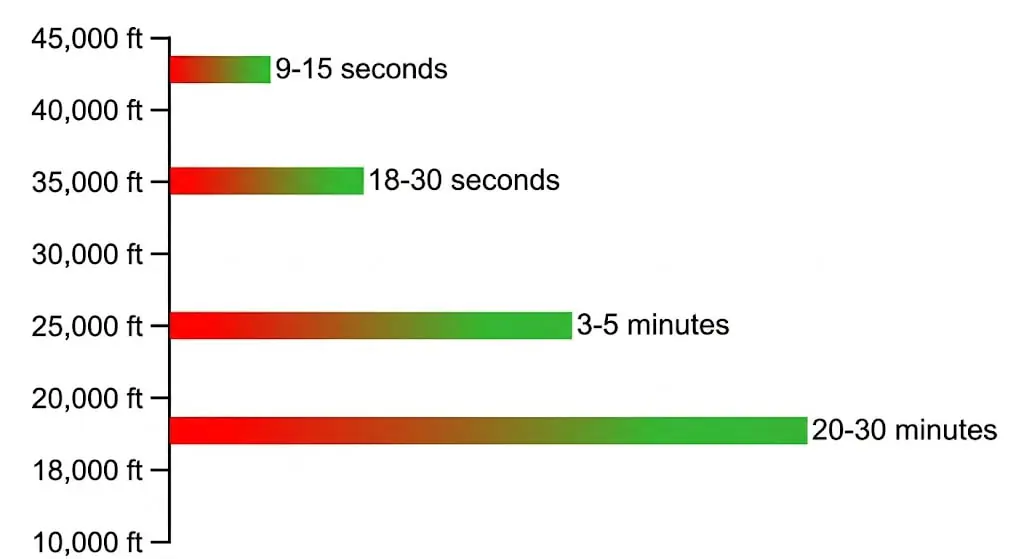
There’s a physiological concept called Time of Useful Consciousness — the window during which a person without supplemental oxygen can still perform purposeful actions. At typical cruise altitudes of 35,000 feet, that window is 18 to 30 seconds after rapid decompression. At 43,000 feet, where some aircraft operate, it drops to 9 to 15 seconds.
This is the number that explains every instruction you’ve ever heard in a safety briefing.
Why fit your mask before helping others? Because if you spend your 18 seconds fitting a mask on a child first, you’ll lose consciousness before finishing — and neither of you ends up protected. Fitting your own mask first isn’t a moral choice. It’s the only sequence that gives you any chance of helping anyone else.
The passenger oxygen system is a chemical generator, not a tank. When the lanyard is pulled, a chemical reaction produces oxygen. The yellow bag that inflates and deflates isn’t a reservoir — it’s a rebreathing bag that captures exhaled air and re-oxygenates it. The system provides 12 to 15 minutes of oxygen. Not because the emergency lasts that long, but because 12 to 15 minutes is exactly how long the crew needs to complete an emergency descent from cruise altitude to below 10,000 feet. The margins are deliberate.
Do not wait for the bag to inflate before breathing. Oxygen flows the moment you pull the mask down. The bag inflating and deflating is normal operation.
What the Crew Does in the First 30 Seconds

The crew response is one of the most precisely trained sequences in aviation — because the TUC window leaves no margin for hesitation.
Both pilots fit their oxygen masks first. Before verifying the cause. Before calling ATC. Before doing anything else. Crew masks are fundamentally different from passenger drop-down masks: they’re full-face pressure-demand units that supply oxygen under positive pressure regardless of ambient cabin pressure. With masks fitted, the pilots declare an emergency on ATC frequency and squawk 7700 on the transponder simultaneously.
Then the emergency descent begins.
Thrust to idle. Speed brakes extended. Nose down. Maximum certified descent rate — typically 4,000 to 6,000 feet per minute for a transport-category aircraft. Target altitude: 10,000 feet, or the Minimum Safe Altitude for that route segment if higher. At 4,000 feet per minute, a descent from 35,000 feet to 10,000 feet takes six minutes. The passenger oxygen system provides 12 to 15 minutes. The sequence is engineered with margin built in.
The emergency descent is the primary life-safety procedure in a rapid decompression event. The masks exist to support the crew during those six minutes of descent. Once the aircraft is below 10,000 feet, the supplemental oxygen requirement ends and the emergency, physiologically speaking, is resolved.
What Causes Rapid Decompression — and What Doesn’t

The events that get public attention — windows shattering, passengers partially ejected, fuselage panels separating — are documented in accident history. But they represent the extreme end of the cause spectrum.
Pressurization system malfunction is the most common cause in commercial operations. Outflow valves failing to close correctly. A pressurization controller fault. An air conditioning pack issue allowing pressure to bleed away faster than it’s replaced. These events are serious, but typically slow enough that the crew has time to respond methodically.
Structural fatigue is the second major cause. Every pressurization cycle — every takeoff and landing — expands and contracts the fuselage slightly. Over thousands of cycles, metal fatigue accumulates at vulnerable points: window frame corners, door surrounds, fuselage skin lap joints. The SKYbrary documentation on cabin pressurisation loss covers the historical event chain in detail. Modern airworthiness directives are specifically calibrated to detect and address fatigue cracks before they reach critical length.
Cargo door failures, improperly latched doors, and window seal degradation complete the primary cause list. Each is manageable through the maintenance inspection and crew door check procedures that exist specifically because these failure modes are known.
Explosive decompression from random structural failure on a well-maintained, modern aircraft is the rarest variant — statistically negligible compared to pressurization system issues.
What I’m Doing While the Crew Is Descending

Going back to that Seoul–Osaka sector event: when the ACARS message arrived, I knew the crew wasn’t going to call me for at least five minutes. They were executing. My job was to have everything ready for the moment they could.
First: terrain. The emergency descent corridor has to be checked for Minimum Safe Altitudes. Some route segments over mountainous terrain can’t safely descend to 10,000 feet without terrain conflict. If that’s the case, I need to identify it for ATC and the crew immediately — because a crew descending blind to 10,000 feet over terrain that requires 12,000 feet is a second emergency on top of the first one. On the Seoul–Osaka sector, the terrain cleared. That’s not always the case on other routes I’ve dispatched.
Second: divert options. I’m building a shortlist of suitable airports along the route — runway length for the aircraft type, fuel remaining after the emergency descent (which burns significantly more than cruise), emergency services availability, and medical facilities if passengers were injured. I’m also considering passenger handling: Does the airport have adequate facilities? Can we get ground support staff there quickly?
Third: coordination. Divert slot with ATC. Station management at the receiving airport. Maintenance inspection arranged before the aircraft lands — because after a rapid decompression, the aircraft does not fly again until the cause is found and cleared. That’s not a policy decision. It’s an airworthiness requirement.
The crew doesn’t need the dispatcher to tell them what to do during the descent. They know. What they need is to get on the radio after leveling at 10,000 feet and hear: “Nearest suitable is [airport], runway 28L, 3,200 meters, emergency services standing by, maintenance on call.” That’s what I build while they’re descending.
In all three cases I’ve tracked, the aircraft diverted safely. In every case, the sequence — crew response, descent, divert — worked exactly the way it was designed.
What Passengers Experience — and What to Do

From the passenger side, rapid decompression is a sudden sensory event: a loud noise, a drop in temperature, and a visible mist or fog filling the cabin as the pressure drops and moisture condenses. It looks alarming. It isn’t smoke.
What to do, in order:
Put your mask on. Immediately. Don’t look around. Don’t check on the person next to you first. You have 18 to 30 seconds at cruise altitude. Mask on, cup over nose and mouth, strap behind your head, pull the tab to tighten. Then assist whoever is next to you.
Stay seated and keep your seatbelt fastened. The emergency descent that follows is steep — the aircraft is descending at rates that would feel extreme even to experienced travelers. Unsecured passengers and objects become projectiles. Your seatbelt should already be fastened; if it isn’t, fasten it now.
Expect noise, cold, and fog. None of these mean the aircraft is failing. The noise is the physics of rapid pressure change. The temperature drop is real — it can be sudden and sharp. The fog is condensation from the cabin air, not smoke or fire. These are normal consequences of the event, not indicators of structural failure.
Follow crew instructions after the descent. Once the aircraft is below 10,000 feet, the crew will instruct you to remove the masks. The aircraft will divert. The flight will not continue to the original destination — structural inspection is mandatory before another pressurization cycle. This is not a decision the airline makes to be cautious. It’s an airworthiness requirement with no exceptions.
The most important thing I’d tell any passenger about rapid decompression is the same thing I’d tell them about any aviation emergency: the system was built to resolve it. The masks buy the time. The descent solves the problem. The divert completes it safely. In 15 years of watching this from the operations side, that sequence has held.
Related Reading from Aeruxo:
- Emergency Landing Explained: What Really Happens and Why It’s Usually Safe
- Airplane Fire Explained: How Aircraft Detect and Handle In-Flight Fire
- Engine Failure on a Plane: What a 15-Year Dispatcher Plans For
Frequently Asked Questions
What is rapid decompression on a plane?
Rapid decompression is a loss of cabin pressurization that occurs faster than the aircraft’s systems can compensate, causing the interior cabin altitude to rise toward the actual outside altitude. It ranges from a pressurization system malfunction producing a gradual pressure loss to an explosive structural failure that equalizes pressure in a fraction of a second. Both trigger the same crew response: oxygen masks on, emergency descent initiated, and divert to the nearest suitable airport.
What is the 18-second rule in aviation?
The 18-second rule refers to the Time of Useful Consciousness at cruise altitudes around 35,000 feet — the window during which a person without supplemental oxygen can still perform purposeful actions after rapid decompression. At higher altitudes, TUC drops to 9 to 15 seconds. This is the physiological reason for fitting your own mask before assisting others: if you spend those 18 seconds on someone else’s mask, neither person ends up protected.
Why do oxygen masks drop from the ceiling during rapid decompression?
Passenger oxygen masks deploy automatically when cabin altitude exceeds approximately 14,000 feet, triggered by a pressure sensor. They provide 12 to 15 minutes of oxygen through a chemical generator — specifically enough time for an emergency descent from cruise altitude to below 10,000 feet. They are not a signal that the aircraft is about to crash. They are the pressurization failure warning and time-buying system that allows the crew to execute the descent safely.
Can a plane window breaking cause rapid decompression?
Yes. Window failures are a documented cause, typically from structural fatigue at window frame corners after thousands of pressurization cycles, or pre-existing cracks from inadequate inspection intervals. Modern airworthiness directives require regular window frame inspection specifically because this failure mode is known and preventable. A window failure produces an extremely loud noise, significant airflow, and rapid pressure change — all survivable if the crew responds correctly and passengers keep their seatbelts fastened.
What causes most rapid decompression events?
The most common cause is pressurization system malfunction — outflow valve failures, air conditioning pack issues, or pressurization controller faults — which typically produce gradual rather than explosive decompression. Structural fatigue at high-cycle stress points is the second major cause. Cargo door failures and improperly latched passenger doors are also documented. Explosive decompression from random structural failure on a well-maintained aircraft is statistically the rarest variant.
What does the dispatcher do during a rapid decompression event?
The moment I’m alerted by ACARS emergency message or transponder squawk 7700, I verify the emergency descent corridor for Minimum Safe Altitudes — critical over mountainous terrain where descending to 10,000 feet may not be safe. Simultaneously I identify suitable divert airports considering runway length, remaining fuel, emergency services, and medical facilities. I coordinate the divert slot, notify station management, and arrange maintenance inspection at the receiving airport — all before the crew can call me, because during the descent they’re executing the checklist and can’t communicate.
Is it safe to fly after a rapid decompression event?
The aircraft that experienced the rapid decompression will not fly again until the cause is identified and rectified — structural inspection is mandatory, and the aircraft is grounded until cleared by maintenance and the relevant aviation authority. Passengers rerouted onto another aircraft are on a completely different airplane with no connection to the event. The investigation that follows a rapid decompression typically results in airworthiness directives applied fleet-wide, improving safety across the entire aircraft type.
Have you experienced an unexpected oxygen mask deployment or a noticeable pressure change on a flight? Share what it felt like in the comments — it helps other passengers understand what actually happens in the cabin.
Disclaimer: The views expressed in this article are my own professional opinions based on 15+ years of operational experience. They do not represent the official position of any airline, aviation authority, or regulatory body.

Licensed Flight Dispatcher with 15+ years of experience in airline operations control. Holds FAA Aircraft Dispatcher Certificate and Republic of Korea Flight Dispatcher License (MOLIT). Specializes in flight watch, NOTAM analysis, flight planning, and operational control at a Korean LCC. IOSA audit participant and author of multiple airline operational manuals, including Emergency Response, De-icing, and OCC Procedures.